



Primary Safety Endpoint
In a real-world female patient population with challenging calcium Shockwave IVL had strong safety outcomes.
| Parameter | Rate |
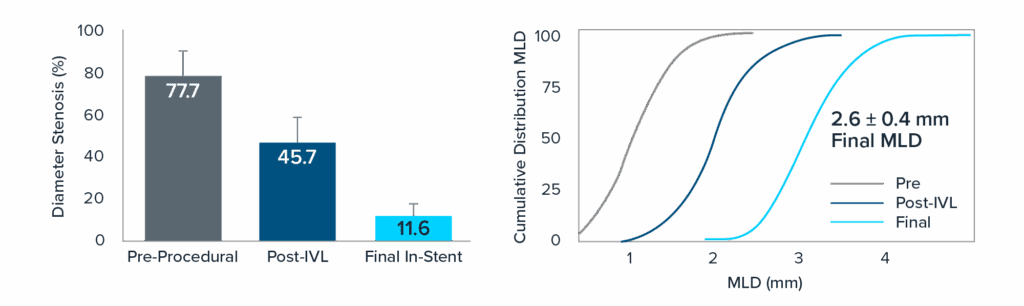
| Target lesion failure within 30-days | 11.6% |
| Cardiac death | 1.0% |
| MI
Peri-procedural MI (<48hrs) Spontaneous MI (>48hrs) |
10.6% 9.6% 1.5% |
| ID-TLR | 1.3% |
SCAI definition used for periprocedural MI. The Fourth Universal definition (Type 4a) used for spontaneous MI beyond discharge.
- Protocol required systematic biomarker collection in all patients.
- MI rate reflective of complex patient population
- Majority of MIs were biomarker elevation alone without clinical symptoms