Impact of SCAI Consensus on Daily Practice: Q&A with Dr. Deepthi Sudhakar
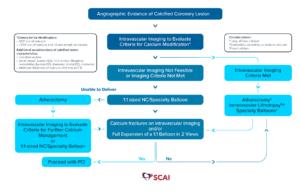
Shockwave Coronary IVL has been included as a device consideration in a SCAI treatment algorithm for concentric, eccentric, focal and nodular coronary calcification. In a first-of-its kind expert consensus statement, the Society for Cardiovascular Angiography and Interventions (SCAI) reinforces Coronary IVL’s consistent, clinically-demonstrated efficacy regardless of calcium morphology.1,2 In addition, the experts conclude that Coronary IVL can be used synergistically with atherectomy devices, especially in balloon uncrossable lesions or longer lesions with heterogeneous calcium and vessel size.
The SCAI Consensus Statement on the Management of Calcified Coronary Lesions3 aimed to create an algorithmic approach to treating calcified coronary artery disease (CAD). The purpose of the publication was to put forth an expert consensus document regarding methods to identify types of calcified coronary lesions, a central algorithm to help guide use of the various calcium modification strategies, tips for when using each treatment modality, and a look at future studies and trials for treating this challenging lesion subset.
In this Q&A, we invited Dr. Deepthi Sudhakar, Sharp Memorial Hospital, San Diego, CA and the Committee Co-Chair of SCAI WIN, to share her insights on the algorithm’s recommendations and its impact on her daily practice.
What was your algorithm before you came across the SCAI Algorithm1?
Dr. Sudhakar: The SCAI expert consensus statement on the management of calcified coronary lesions provides valuable guidance on the management of severely calcified lesions, which are amongst the most challenging cases we encounter. With all the tools now available for plaque modification and variability in lesion types, this document distills the management of a complex subset of lesions into a streamlined algorithm. I frequently use intravascular imaging for guiding lesion preparation; however, since reviewing this algorithm, I have increased my use of imaging after modification to assess adequacy. I have also increased the use of more than one tool for lesion preparation.
How important is it to have society guidance on things like calcium specifically?
Dr. Sudhakar: We are seeing increasingly higher rates of complex calcified lesions and restenosis lesions, and this, coupled with the advancement of new technologies for plaque modification, has led to a lot of heterogeneity in our understanding and management of these lesions. The publication of this statement is well-timed and serves a need for a thoughtful, standardized approach to these lesions. Importantly, it highlights that not all calcified lesions are created equal, and modification is not a one-size-fits-all approach. There is a lot of emphasis placed on imaging to understand the subset of calcified lesions before deciding on a modification strategy. This is key to choosing the most appropriate modification strategy for better long-term outcomes. It is comprehensive and encompasses several types of lesions, such as bifurcation lesions and chronic total occlusions.
Is there anything you’d change or add to the current algorithm?
Dr. Sudhakar: Expand on the subsets of lesions where you might want to combine different modalities for calcium modification. The scarcity of existing data limits some of this, so it will be very interesting to see how the results of ongoing trials like ECLIPSE (NCT03108456), ROLLING-STONE (NCT05016726), SHORT-CUT (NCT06089135), and ROLLERCOASTR (NCT04181268) add to our understanding of modification. The addition of restenosis lesions to the algorithm would also be helpful. While more tools are available for calcium modification, not all are widely available. I think that is an important aspect to keep in mind when adopting any algorithm. The setting where lesion preparation occurs and hemodynamics are also important factors to remember.
How important is imaging in your algorithmic approach to calcium?
Dr. Sudhakar: Imaging is crucial in any percutaneous coronary intervention, especially with calcified lesions. As the document clearly states, multiple calcified lesions and outcomes vary despite adequate preparation in some cases, such as eruptive nodules. We must understand what we are treating specifically before choosing the right modality. This is particularly true in restenosis lesions, where understanding the mechanism is critical to lesion preparation.
Was there anything about your approach or a device that the SCAI Algorithm changed?
Dr. Sudhakar: I frequently use intravascular imaging; however, this document led me to focus on more aspects of a lesion outside of arc length, such as the type of calcified nodule and depth of calcium. I have also increased my use of imaging after lesion preparation to ensure fracture and check for dissections in eccentric lesions. In contrast, before the document, I relied more often on expansion with non-compliant balloons after modification to determine the adequacy of preparation. I have also increased my use of combining atherectomy with intravascular lithotripsy in treating these lesions.
Are there any challenges you encounter with calcium that may not have a current treatment paradigm?
Dr. Sudhakar: Bifurcation lesions with severe calcification and restenosis lesions with protrusion of calcified nodules remain challenging subsets to treat.
Do you follow a mental step-by-step process, and if so, when does that kick in? After imaging or upon visualization by angio?
Dr. Sudhakar: A patient’s age and underlying comorbidities are factors I consider even before the initial angiogram in forming my pre-test probability of calcified disease. On the initial angiogram, I am focusing on calcification, tortuosity at the lesion, the presence of bifurcation lesions, and estimates of vessel size. Calcification on angiography, particularly if there are eccentric lesions, shows me that I need to assess for calcified nodules when imaging. I rely on intravascular imaging to guide my modification strategy. Still, my decision also heavily depends on the patient’s characteristics, hemodynamics, and ability to tolerate one modification tool versus another.
What data do you think are still needed to verify or support the algorithm?
Dr. Sudhakar: We have some data to support the use of atherectomy with intravascular lithotripsy; however, there needs to be long-term data, which the ongoing trials should shed some light on. Sex differences in how we treat calcified lesions are another area where we lack data, which calls for increasing enrollment in clinical trials. In this regard, EMPOWER (NCT05755711) may be able to shed some light on this topic.
Dr. Deepthi Sudhakar is a paid consultant of Shockwave Medical.
1: Ziad Ali et al. “Safety and Effectiveness of Coronary Intravascular Lithotripsy for Treatment of Calcified Nodules.” JACC Cardiovasc Interv. 2023.
2: Ziad Ali et al. “Impact of Calcium Eccentricity on the Safety and Effectiveness of Coronary Intravascular Lithotripsy: Pooled Analysis From the Disrupt CAD Studies.” Cardiovascular Interv. 2023.
3: Riley, Robert F., Mitul P. Patel, J. Dawn Abbott, Sripal Bangalore, Emanouil S. Brilakis, Kevin J. Croce, Darshan Doshi, et al. “SCAI Expert Consensus Statement on the Management of Calcified Coronary Lesions.” Journal of the Society for Cardiovascular Angiography & Interventions 3, no. 2 (February 2024): 101259. https://doi.org/10.1016/j.jscai.2023.101259.
Shockwave IVL: In the U.S.: Rx only. Prior to use, please reference the Important Safety Information for more information on indications, contraindications, warnings, precautions and adverse events.