DISRUPT PAD III Randomized Clinical Trial
Shockwave Intravascular Lithotripsy (IVL) provides superior vessel prep and excellent long-term results in calcified vessels while preserving future treatment options.
Key Findings
-
Superior Prep
Shockwave IVL’s unique mechanism of action (MOA) delivers significantly more luminal gain with lower dilation pressure and significantly lower dissections. -
Preserved Options
Shockwave IVL maintains control of the procedure by minimizing complications such as dissections, embolization and perforations. Shockwave IVL significantly reduces the need for bailout stents, preserving future treatment options. -
Excellent Long-term Results
Shockwave IVL has demonstrated excellent patency out to two years in a severely calcified patient population.
Study Design & Characteristics
Objective:
To assess safety and effectiveness of IVL versus percutaneous transluminal angioplasty (PTA) as a vessel preparation strategy prior to definitive treatment with drug-coated balloon (DCB) +/- stent in patients with calcified femoropopliteal lesions
Design:
- Prospective
- Multicenter
- Single-blind
- Randomized clinical trial (RCT)
Primary Endpoint:
- Procedural success (residual stenosis ≤ 30% without flow-limiting dissection)
Powered Secondary:
- Primary patency at one year (freedom from clinically driven target lesion revascularization (CD-TLR) + freedom from restenosis determined by duplex ultrasound (US) + freedom from provisional stenting)
306 superficial femoral artery (SFA)/popliteal lesions
83% severe calcification*; 129 mm* average calcified length
*IVL Arm
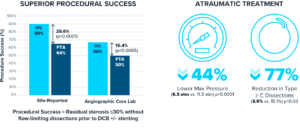
Superior Prep
Shockwave IVL’s unique MOA delivers significantly more luminal gain with lower dilatation pressure and less need for post-dilatation.
Preserved Options
Shockwave IVL maintains control of the procedure by minimizing complications such as dissections, embolization and perforations. Shockwave IVL significantly reduces the need for bailout stents, preserving future treatment options.
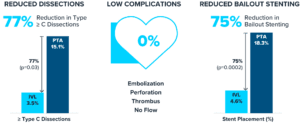
- Embolic protection: Utilized in 1.3% of cases in Shockwave IVL treatment arm
- Provisional stent: Utilized if residual stenosis ≥50% by visual estimate or unresolved ≥ type D dissection, and trans-lesional gradient > 10 mmHg
Excellent Long-term Results
Shockwave IVL has demonstrated excellent patency out to two years in a severely calcified patient population.
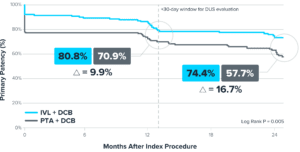
Number of subjects at risk:
| Months After Index Procedure | 0 | 6 | 12 | 18 | 24 |
|---|---|---|---|---|---|
| Shockwave IVL | 131 | 120 | 107 | 88 | 83 |
| PTA | 136 | 107 | 95 | 75 | 66 |
*Primary patency defined as freedom from provisional stenting at index procedure, freedom from clinically-driven target lesion revascularization, and freedom from restenosis determined by duplex ultrasound.
Conclusion
-
DISRUPT PAD III compared endovascular therapy of IVL to percutaneous transluminal angioplasty (PTA) for treatment of calcified peripheral arteries.
-
Results validate Shockwave IVL as a safe and effective treatment for heavily calcified femoropopliteal lesions.
-
Shockwave IVL provides superior vessel prep and excellent long-term results in calcified vessels while preserving future treatment options.
Study Leadership
This section contains attributions including profile pictures, titles, descriptions, and Twitter handles.
-
Gunnar Tepe, MDProfessor of Radiology, Head of Diagnostic & Interventional Radiology, RoMed Clinic, Rosenheim, Germany
-
Marianne Brodmann, MDHead of Division of Angiology, Medical University Graz, Graz, Austria
-
William Bachinsky, MDCardiologist, Penn State Health Holy Spirit Medical Center, Mechanicsburg, PA
-
Sahil. A Parikh, MDAssociate Professor of Medicine, Columbia University, New York, NY
-
William A. Gray, MDProfessor of Medicine, Main Line Health, Wynnewood, PA
Tepe et al Intravascular Lithotripsy for Peripheral Artery Calcification: Mid-term Outcomes From the Randomized Disrupt PAD III Trial. JSCAI, Volume 1, Issue 4, 100341.
Tepe et al Intravascular Lithotripsy for Peripheral Artery Calcification 30-Day Outcomes From the Randomized Disrupt PAD III Trial JACC Cardiovasc Interv. 2021 Jun 28;14(12):1352-1361.
More Clinical Evidence
-
This DISRUPT BTK II sub-analysis focuses on results from the CLTI cohort at 12-months.Peripheral IVL
-
Global prospective, multi-center, single-arm study assessing the safety and effectiveness of Shockwave peripheral IVL in treating long, calcified BTK lesions.Peripheral IVL
-
The largest prospective real-world evidence for the treatment of complex, heavily calcified peripheral arterial disease (PAD).Peripheral IVL