Case Reviews
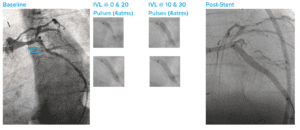
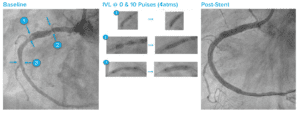
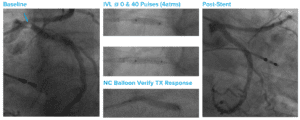
Highly Angulated Calcified LCX With Lesions Proximal and Distal
Case submitted by Javier Escaned, San Carlos Hospital
Summary: Highly angulated left circumflex artery (LCX) with lesions proximal and distal; OCT wouldn’t cross either lesion; guideliner-assisted Shockwave IVL catheter delivery followed by successful IVL therapy; the case was completed with easy deployment of two long drug-eluting stents (DES).