Enhanced Deliverability with Shockwave C2 Aero in Complex Coronary Lesions with Dr. Brett Wanamaker
Dr. Brett Wanamaker, MD, FACC, FSCAI, Associate Professor of Internal Medicine at the University of Michigan, presents a Shockwave C2 Aero case demonstrating improved deliverability and crossability in complex calcified coronary lesions.
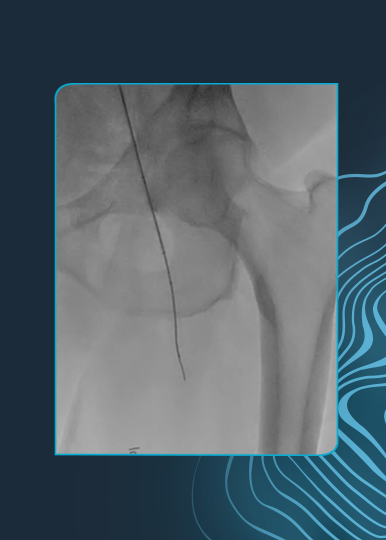
Treating Complex Calcified LAD and RCA CTO Lesions
This case highlights treatment of a severely calcified left anterior descending artery (LAD) and a right coronary artery (RCA) chronic total occlusion (CTO). The Shockwave C2 Aero successfully crossed a tortuous proximal LAD and the RCA CTO with minimal guidewire or catheter support, demonstrating strong lesion crossing capability in challenging anatomy.
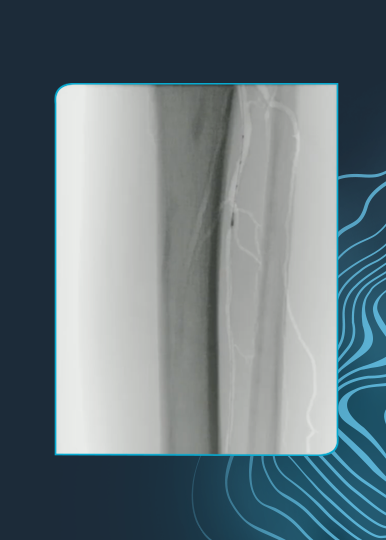
Overcoming Failed Stent Delivery
Although noncompliant balloons were able to cross both lesions, initial stent delivery attempts were unsuccessful—highlighting the limitations of conventional approaches in heavily calcified lesions.
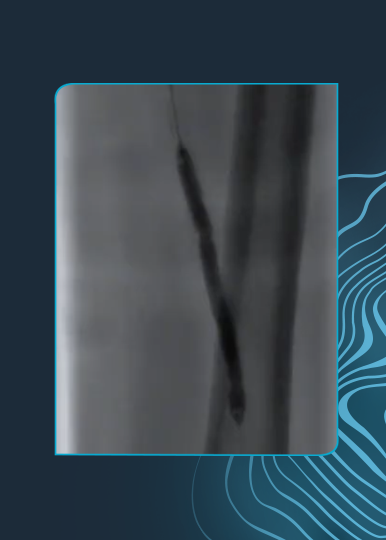
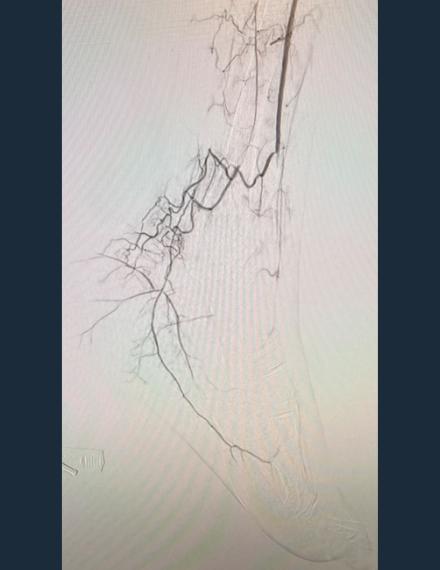
Enabling Stent Delivery with Calcium Modification
Following calcium modification with Shockwave C2 Aero, stent delivery was achieved. Final imaging confirmed strong stent expansion with a high minimal stent area (MSA), supporting a favorable procedural outcome and positive patient prognosis.
Watch the full case review to see how Shockwave C2 Aero improves crossability, enables stent delivery, and optimizes outcomes in complex calcified coronary lesions.
Dr. Wanamaker is a paid consultant of Shockwave Medical.
Shockwave IVL: In the U.S.: Rx only. Prior to use, please reference the Important Safety Information for more information on indications, contraindications, warnings, precautions and adverse events.