DISRUPT BTK II CLTI Cohort Analysis
Count on it: New data validates Shockwave Intravascular Lithotripsy’s (IVL) impact on patients with chronic limb threatening ischemia (CLTI) at 12 months. DISRUPT BTK II assessed the continued safety and effectiveness of the Shockwave Peripheral IVL System for the treatment of calcified, stenotic lesions in below-the-knee (BTK) arteries. This sub-analysis focuses on results from the patients with CLTI enrolled in the study.
CLTI Cohort Key Findings
-
Wound Healing
In a majority of patients with CLTI, IVL plays a critical role in laying the foundation for successful wound healing through safe and effective revascularization. -
Limb Salvage
12-month outcomes establish IVL’s role in limb salvage and enabling functional recovery in patients with CLTI. -
Frontline Strategy
The DISRUPT BTK II 12-month data establishes IVL as a frontline calcium modification* for complex BTK lesions, delivering outcomes that redefine the benchmark for success in the treatment of patients with CLTI.
Armstrong E, VIVA 2025. Data on file at Shockwave Medical.
*Frontline strategy: The approach of utilizing IVL as the primary treatment method, implemented without the use of atherectomy. This strategy is backed by the DISRUPT BTK II data based on the percentage of procedures involving pre-dilatation and post-dilatation, as well as the proportion of stenting performed. Our BTK II data indicates a notably low usage of both pre-dilatation and post-stenting in these cases. The majority of patients enrolled had CLTI, thus a majority of the comorbidities are attributed to this population.
DISRUPT BTK II Study Design
Objective
Assess the continued safety and effectiveness of the Shockwave Medical Peripheral IVL System for the treatment of calcified, stenotic lesions in BTK arteries. Products included Shockwave M5+ and Shockwave S4.
Key Inclusion Criteria
- Rutherford classification (RC) 3-5, RC 3 capped at 20% of enrolled patients
- Moderate-severe calcification*
- Up to two BTK lesions ≤ 200 mm in length
Primary Safety Endpoint
Major adverse limb events (MALE) or post-operative death (POD) at 30 days
Primary Effectiveness Endpoint
Procedural success, defined as ≤ 50% residual stenosis for all treated target lesions without serious angiographic complications
Additional analysis to include lesions with ≤ 30% residual stenosis without angiographic complications
Independent Clinical Events Committee (CEC), Angiographic Core Laboratory, and Duplex Ultrasound Core Laboratory
The DISRUPT BTK II study enrolled the largest cohort of real-world, complex patients* with moderate to severe calcium below the knee
DISRUPT BTK II sets a new benchmark for what’s possible for the challenging lesions. No other technology has been evaluated in such severely calcified BTK lesions to date
*Presence of fluoroscopic evidence of calcification by PARC (Peripheral Academic Research Consortium) definition: 1) on parallel sides of the vessel and 2) extending > 50% the length of the lesion if lesion is ≥ 50 mm in length; or extending for minimum of 20 mm if lesion is < 50 mm in length.
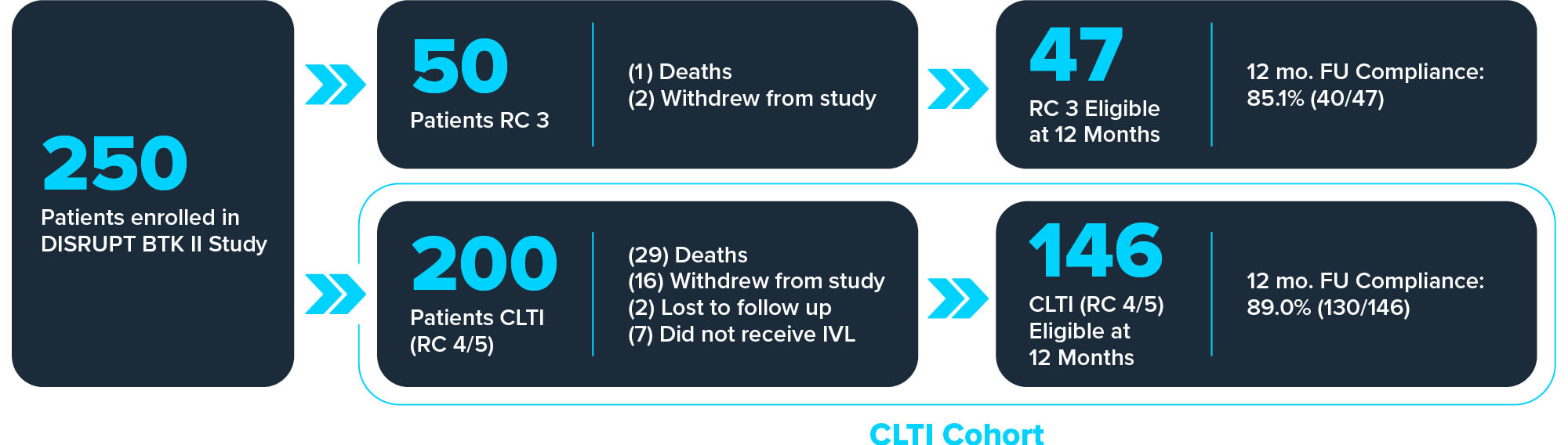
Full Cohort By the Numbers
Statistics Callout
This section presents key statistical information with numbers and descriptions.
-
250Patients
-
305Lesions
-
38Global sites
-
2Year follow-up
Armstrong E, VIVA 2025.
CLTI Cohort By the Numbers
Statistics Callout
This section presents key statistical information with numbers and descriptions.
-
200Patients
-
245Lesions
CLTI Cohort Baseline Demographics
Rutherford Category
Statistics Callout
This section presents key statistical information with numbers and descriptions.
-
71%RC 5, minor tissue loss2*
-
29%RC 4, ischemic rest pain2**
Medical History
Statistics Callout
This section presents key statistical information with numbers and descriptions.
-
73%Patients had wounds at baseline2
-
18%Hemodialysis-dependent1
-
77%Diabetes mellitus1
Lesions
Statistics Callout
This section presents key statistical information with numbers and descriptions.
-
86%Moderate-severe Ca++1†
-
80mmMean lesion length1
-
31%Chronic total occlusions (CTOs)1
1: Armstrong E, VIVA 2025.
2: Data on file at Shockwave Medical.
*Per limb 143/201 | **Per limb 59/201 | †PARC Definition
Results and conclusion
Clinical Procedural Insights in a CLTI Cohort
In a challenging patient cohort, IVL was shown to be a safe and effective treatment of challenging calcific BTK lesions with minimal need for provisional stenting.
CONFIRMED SAFETY
| Total Serious Angiographic Complications Post-IVL2 | Total Serious Angiographic Complications at Final1 |
| 2.3% | 1.3% |
CONFIRMED EFFECTIVENESS
| Average Residual Stenosis Post-IVL2 | Average Residual Stenosis at Final1 |
| 30.0% | 25.7% |
MINIMAL PROVISIONAL STENTING
| Stent/Tack Implant Total2 | Provisional Stent/Tack Implant2 |
| 5.7% | 2.8%* |
*Remaining Stent/Tack implants were part of physicians’ standard algorithm.
1: Armstrong E, VIVA 2025.
2: Data on file at Shockwave Medical.
Freedom from CD-TLR and Patency at 12 Months
12-month outcomes confirm the durability of IVL through sustained vessel patency and low reintervention rates which lead to limb preservation and ongoing symptom relief.
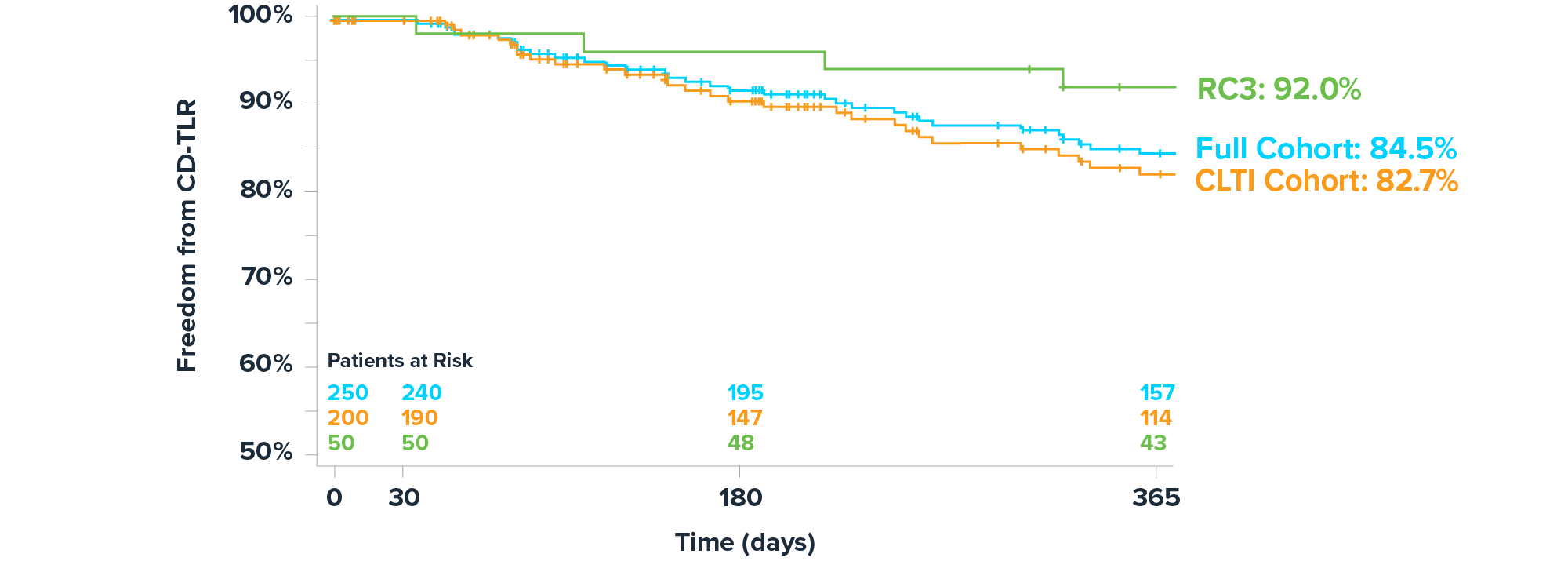
| Rutherford Category | Freedom from CD-TLR at 12 Months |
| Full Cohort (n=250) | 84.5%1 |
| RC 3 (n=50) | 92.0%1 |
| CLTI Cohort (n=200) | 82.7%1 |
| RC 4 (n=57) | 88.0%2 |
| RC 5 (n=143) | 80.3%2 |
| Patency at 12 Months (CLTI) | |
| 64.0% (n=80/125)1 | |
1: Armstrong E, VIVA 2025.
2: Data on file at Shockwave Medical.
Clinically driven target revascularization (CD-TLR).
Kaplan Meier (KM) is an analysis that uses probability to capture patients lost to follow-up.
Freedom from CD-TLR analysis excluded patients with above the ankle amputation of target limb.
Freedom from Major Amputation at 12 Months
12-month outcomes establish IVL’s role in limb salvage and enabling functional recovery in patients with CLTI.
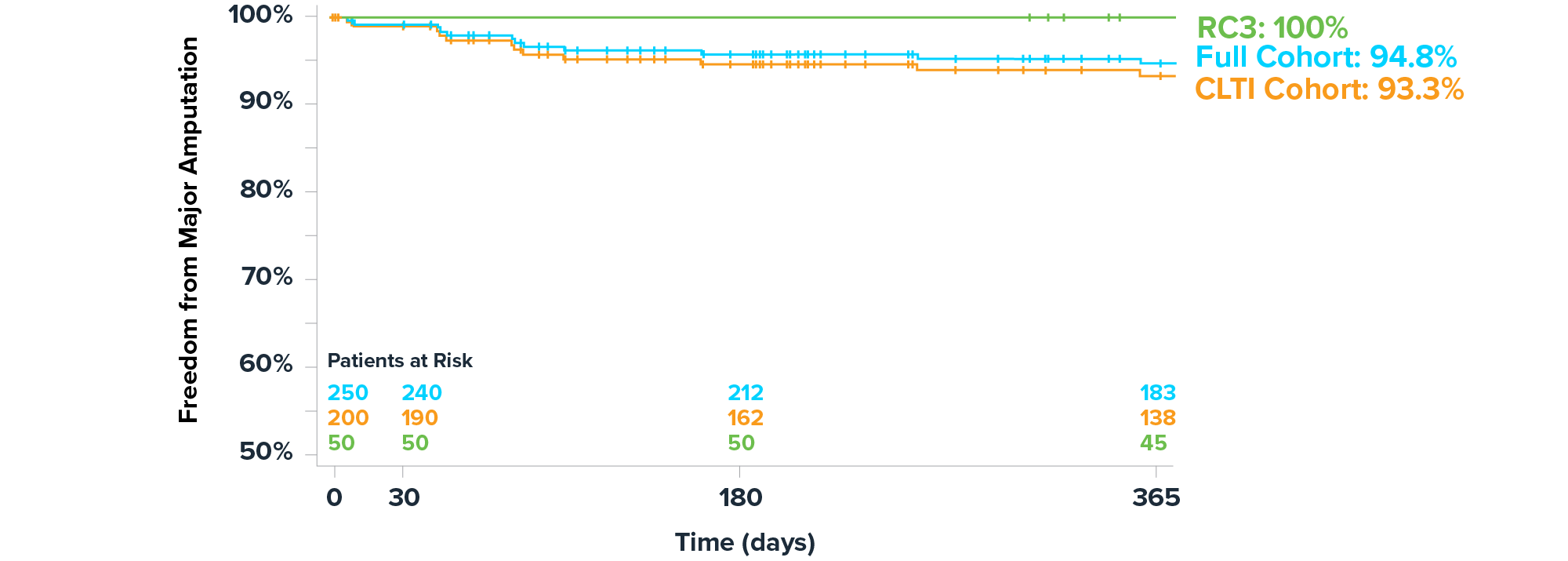
| Rutherford Category | Freedom from Major Amputation at 12 Months |
| Full Cohort (n=250) | 94.8%1 |
| RC 3 (n=50) | 100%1 |
| CLTI Cohort (n=200) | 93.3%1 |
| RC 4 (n=57) | 98.1%2 |
| RC 5 (n=143) | 91.2%2 |
1: Armstrong E, VIVA 2025.
2: Data on file at Shockwave Medical.
Rutherford Classification (RC) Change at 12 Months
IVL played a critical role in laying the foundation for successful wound healing in patients with CLTI through safe and effective revascularization.
- Of the patients remaining at 12 months, 68% were no longer CLTI1
- 61% of wounds were healed or improving1*
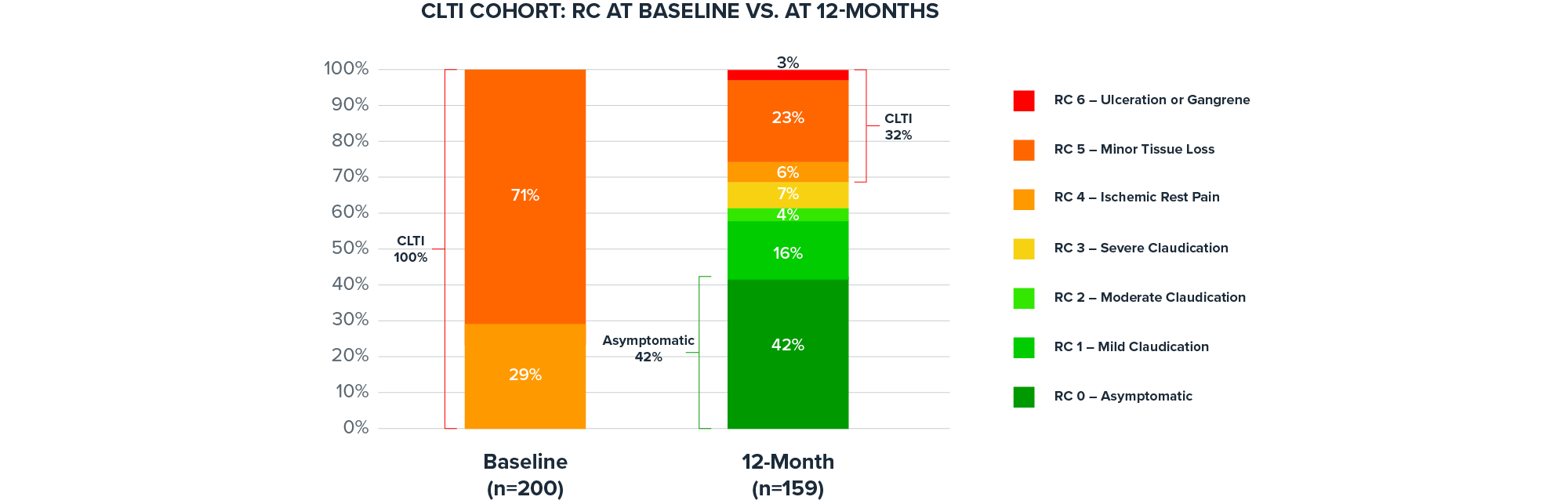
1: Data on file at Shockwave Medical.
Available data is 159 limbs out of 200 limbs of patients with CLTI.
*Mean wound follow up time: 157 days.
Quality of Life at 12 Months
As part of revascularization, IVL facilitates sustained symptom improvement for patients with CLTI through 12 months.
| Breakdown by Attribute | VascuQoL-6 Attribute | Activity | Tired | Walk | Concern | Social | Pain |
| Average Score 12 Months | 2.8 | 2.6 | 3.0 | 2.9 | 3.1 | 2.8 | |
| Average Score Baseline | 1.9 | 2.0 | 2.3 | 1.7 | 2.3 | 1.8 |
All categories improved. Total VascuQoL-6 Score (CLTI) at 12 months significantly improved from baseline (P-Value: p<0.001). Total at 12 months was 17.2 ± 5.0 and total at baseline was 11.9 ± 4.0.1
The Vascular Quality of Life Questionnaire is a survey used to determine health related quality of life (HRQoL) in patients with peripheral arterial disease (PAD). Each attribute is scored 1-4, a higher value indicates better health status. The sum of each individual attribute score is used to generate a total quality of life score.
1: Armstrong E, VIVA 2025.
Study Leadership
This section contains attributions including profile pictures, titles, descriptions, and Twitter handles.
-
Venita Chandra, MDClinical Associate Professor of Surgery, Associate Program Director – Vascular Surgery, Medical Director Stanford Advanced Wound Center
-
Ehrin Armstrong, MDMedical Director, Aurora Denver Cardiology Associates, Swedish Medical Center
More Shockwave Peripheral IVL Studies
-
Global prospective, multi-center, single-arm study assessing the safety and effectiveness of Shockwave peripheral IVL in treating long, calcified BTK lesions.Peripheral IVL
-
The largest-ever randomized clinical study of Shockwave peripheral IVL treatment in severely calcified peripheral lesions, out to 24 months.Peripheral IVL
-
The largest prospective real-world evidence for the treatment of complex, heavily calcified peripheral arterial disease (PAD).Peripheral IVL