DISRUPT PAD II
Core lab adjudicated, long-term, multi-center study exclusively enrolling heavily calcified lesions building upon DISRUPT PAD I. Designed to assess the safety and performance of Shockwave IVL as stand-alone treatment among eight centers in Europe and New Zealand in 2015.

Study Leadership
This section contains attributions including profile pictures, titles, descriptions, and Twitter handles.
-
Marianne Brodmann, MDCo-Principal Investigator Division of Internal Medicine Medical University Graz, Graz, Austria
-
Thomas Zeller, MDCo-Principal Investigator Universitäts-Herz-Zentrum Freiburg-Bad Krozingen, Bad Krozingen, Germany
PAD II Study Details
Statistics Callout
This section presents key statistical information with numbers and descriptions.
-
60Patients with heavily calcified femoral-popliteal lesions
-
85%Severe calcification by PARC¹†
-
98mmAverage calcified length
-
12Month follow-up
1: Brodmann M et al, Primary outcomes and mechanism of action of Intravascular Lithotripsy in calcified, femoropopliteal lesions: Results of DISRUPT PAD II, Catheter Cardiovasc Interv. 2018
†PARC: Peripheral Academic Research Consortium
Compelling Safety & Performance in Severely Calcified Lesions*
Statistics Callout
This section presents key statistical information with numbers and descriptions.
-
0%Perforations, embolization, thrombus, no reflow, abrupt closure
-
1.7%Dissection (D/E/F)**, provisional stenting
-
24%Residual stenosis with average acute gain of 3.0 mm, average balloon inflation pressure of 6 atm after Shockwave IVL therapy
-
100%Procedural success, low use of adjunctive tools
-
79%Freedom from clinically-driven target lesion revascularization (CD-TLR) at one year, with simple revascularization procedures
*Core Lab and Clinical Events Committee (CEC) adjudicated
**Guidewire induced through recanalization of a chronic total occlusion resolved with stent placement
Patients Who Were Treated with Optimal Technique Had Less Than 9% CD–TLR At 12-Months
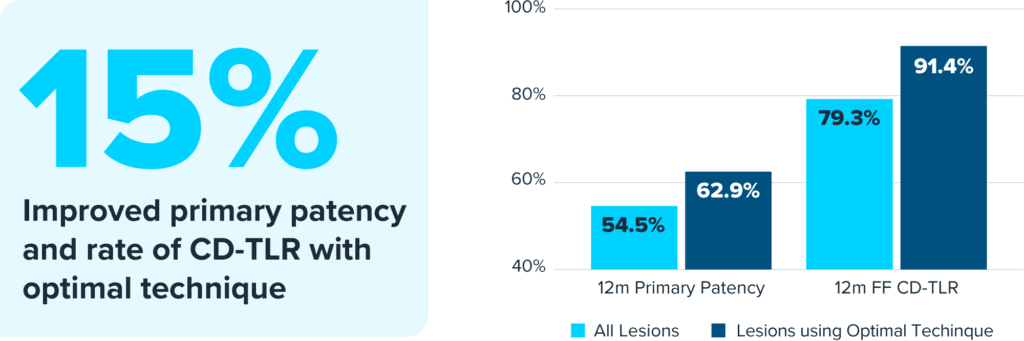
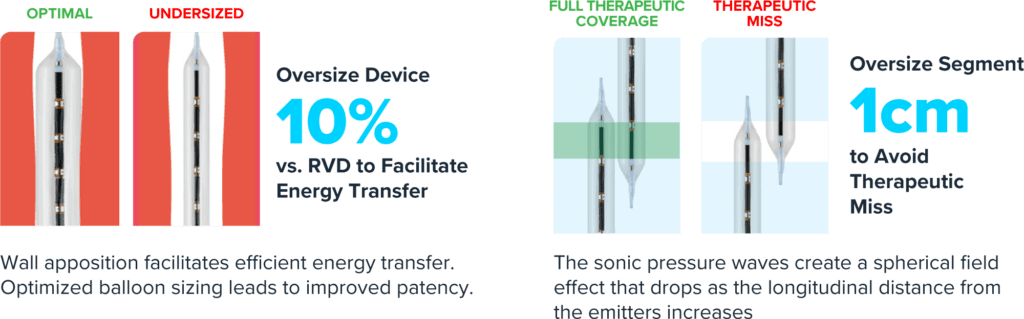
Balloon Sizing and Therapeutic Overlap Enables Optimal Energy Delivery to Peripheral Calcified Lesions
More Shockwave Peripheral IVL Studies
-
Global prospective, multi-center, single-arm study assessing the safety and effectiveness of Shockwave peripheral IVL in treating long, calcified BTK lesions.Peripheral IVL
-
The largest-ever randomized clinical study of Shockwave peripheral IVL treatment in severely calcified peripheral lesions, out to 24 months.Peripheral IVL
-
The largest prospective real-world evidence for the treatment of complex, heavily calcified peripheral arterial disease (PAD).Peripheral IVL