Case Reviews
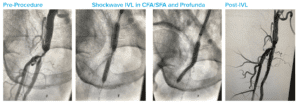
High Risk CFA and Profunda Treatment
Case submitted by Nelson Bernardo, MD, MedStar Health
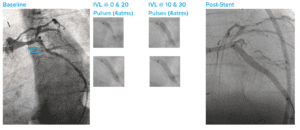
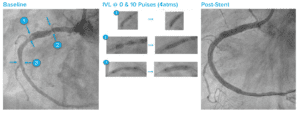
Summary: Patient was considered high surgical risk due to severity of calcium and involvement of profunda. Shockwave IVL treatment of common femoral artery (CFA) and proximal superficial femoral artery (SFA), followed by treatment of profunda with the same device. Final result shows no dissection, perforation, emboli, need for additional devices and full resolution of symptoms.