Case Reviews
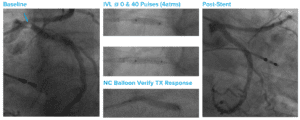
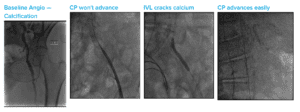
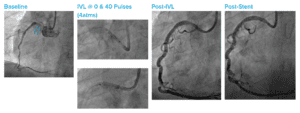
Large Focal Chunk of Eccentric Calcium at the LCX Ostium Into the LM
Case submitted by Antonio Colombo, San Raffaele
Summary: Large eccentric lesion at left circumflex (LCX) ostium; delivered four cycles with 3.5 mm Shockwave IVL catheter; full balloon expansion (and associated lower endoflator pressure) were noted; verified treatment response using a non-compliant balloon; then used the same IVL device to successfully treat the left main (LM).