Shockwave IVL & Concentric Calcium
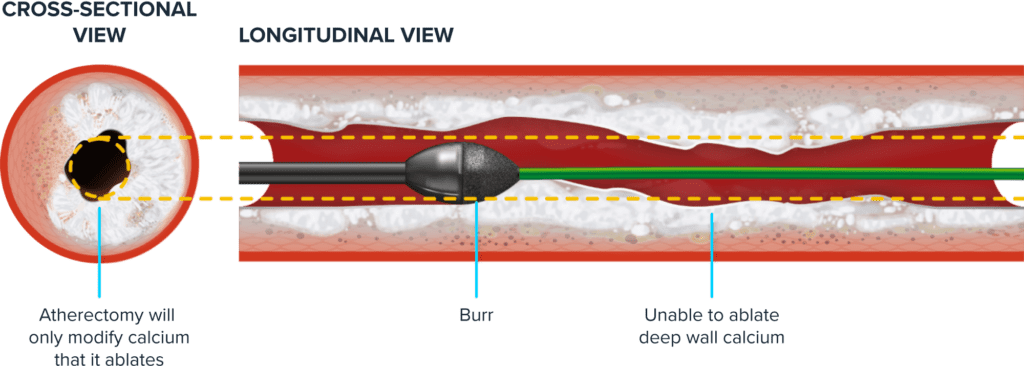
A sound success: Shockwave Intravascular Lithotripsy (IVL) cracks deep into the calcium wall, helping to overcome the limitations of traditional atherectomy ablation on concentric calcium.
Shockwave IVL for Coronary Artery Disease
Shockwave IVL & Eccentric Calcium
Shockwave IVL & Nodular Calcium
Shockwave C2+

Gain the Upper Hand Over Concentric Calcium with Shockwave IVL
Concentric calcium with an arc of greater than 270° can be difficult to treat through alternative calcium modification strategies. Shockwave IVL, on the other hand, has mechanistic advantages which create circumferential, longitudinal and transverse fractures throughout both superficial and deep calcium.
ATHERECTOMY THERAPY:
SHOCKWAVE IVL THERAPY:

Shockwave IVL’s Effectiveness in Concentric Calcium
In this concentric calcium case, large multi-plane and longitudinal calcium fractures were visualized post-Shockwave IVL treatment.
-

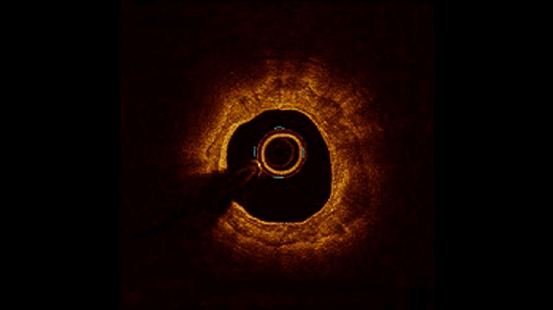
Severe Calcific Stenosis
OCT demonstrating severe calcific stenosis -
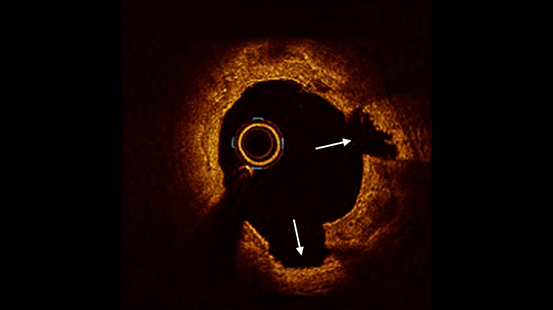
Post IVL
Following Shockwave IVL, two fractures (white arrows) are seen associated with luminal gain -
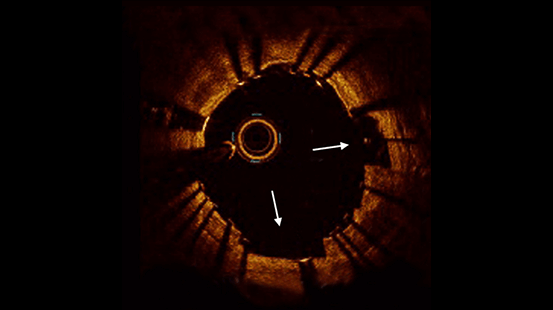
Following Stent Deployment
Fracture widening (markers) following stent deployment facilitates further luminal gain
OCT Analysis in Concentric Calcium Demonstrated Large Minimum Stent Areas and Stent Expansion Post-Shockwave IVL and Stenting
| Pre-IVL (N=66) | |
| Max continuous calcium arc, ° | 360° |
| Lesion length, mm | 32.6 (24.0 to 39.6) |
| Calcium length, mm | 27.0 (18.8 to 34.0) |
| Minimal lumen area, mm2* | 1.97 (1.43 to 2.34) |
| Area stenosis, % | 73.07±12.49 |
| Post-stent at Max Calcium Site (N=66) |
|
| Area stenosis, % | −17.7 (−29.1 to 4.4) |
| Stent area, mm2 | 8.09 (6.77 to 9.03) |
| Stent expansion, % | 102.0 (88.8 to 117.1) |
| Acute area gain, mm2 | 4.70 (3.35 to 6.47) |
| Calcium fracture | 81.8% (54/66) |
| Post-PCI Final Complications |
|
| Severe dissection (D-F) | 0.0% (0/66) |
| Slow flow or no reflow | 0.0% (0/66) |
| Abrupt closure | 0.0% (0/66) |
| Perforation | 0.0% (0/66) |
*MLA was never co-localized with the pre-IVL maximum calcification.
1: Ali et al. Impact of Calcium Eccentricity on the Safety and Effectiveness of Coronary Intravascular Lithotripsy: Pooled Analysis From the Disrupt CAD Studies. Cir Interventions. 2023.
Conclusions from the OCT Pooled Analysis in Concentric Lesions
-
The present individual patient data pooled analysis of 4 studies (N=262) represents the largest evaluation of Shockwave IVL by OCT
-
No serious angiographic complications were observed confirming the safety of Shockwave IVL for the treatment of severely calcified coronary lesions
-
OCT demonstrated extensive calcium fracture after Shockwave IVL treatment with excellent stent expansion of severely calcified lesions
-
Visible calcium fracture and calcium characteristics were not predictors of stent expansion following treatment with Shockwave IVL
Review the full OCT presentation:
Featured Clinical Evidence
-
The largest systematic assessment of Shockwave coronary Intravascular Lithotripsy (IVL) to date based on individual patient data from DISRUPT CAD I–IV.Coronary IVL
-
Individual patient data pooled from DISRUPT CAD I-IV to see Shockwave IVL outcomes, fracture analysis and stent expansion predictors.Coronary IVL
-
The first prospective, female-only study of coronary interventions in complex calcific disease, in collaboration with female leaders.Coronary IVL
-
Shockwave IVL & Eccentric Calcium
Learn how Shockwave IVL successfully modifies eccentric calcium.
-
Shockwave IVL & Nodular Calcium
Learn how Shockwave IVL successfully modifies nodular calcium.