Shockwave IVL Below the Knee
Raise your expectations for below-the-knee (BTK) outcomes. Shockwave Intravascular Lithotripsy (IVL) cracks the complexity of BTK calcium with safe, effective treatment that extends to remarkable lengths.
Shockwave IVL for Peripheral Artery Disease
Shockwave Peripheral IVL Reimbursement
Shockwave E8
Shockwave M5+

Take Below-the-Knee (BTK) Treatment Above and Beyond
The challenges of BTK are made worse by stubborn calcium, with therapies challenged by dissections,1 poor vessel expansion2 and acute recoil.3 With Shockwave IVL, you can safely modify both superficial and deep calcium at ultra-low pressures that won’t impact soft tissue4 — plus our mechanism of action (MOA) is specifically built to treat BTK arteries.
1 Fitzgerald et al, Contribution of localized calcium deposits to dissection after angioplasty. An observational study using intravascular ultrasound, Circulation 1992.
2 Rocha-Singh et al, Peripheral arterial calcification: prevalence, mechanism, detection, and clinical implications, Catheter Cardiovasc Interv, 2014.
3 Baumann et al, Early recoil after balloon angioplasty of tibial artery obstructions in patients with critical limb ischemia, J Endovasc Ther 2014.
4 Kereiakes, DJ, Virmani, R, Hokama JY, et. al. Principles of intravascular lithotripsy for calcific plaque modification. J Am Coll Cardiol Intv 2021.
Shockwave IVL Proven Safe and Effective in Patients with CLTI
Accordion Section
Core Lab Adjudicated
| Complications | Post-IVL N=394 |
Final N=482 |
| Dissections D-F | 1.8% | 0.8% |
| Perforation | 0% | 0.4% |
| Distal Emboli | 0.3% | 0% |
| Slow Flow/No Reflow | 0.3% | 0% |
| Abrupt Closure | 0% | 0% |
1: Intravascular Lithotripsy for the Treatment of Patients with Critical Limb Ishemia, Peter A. Soukas, MD. Presented at The Amputation Prevention (AMP) Symposium. Chicago, IL. USA, August 2022.
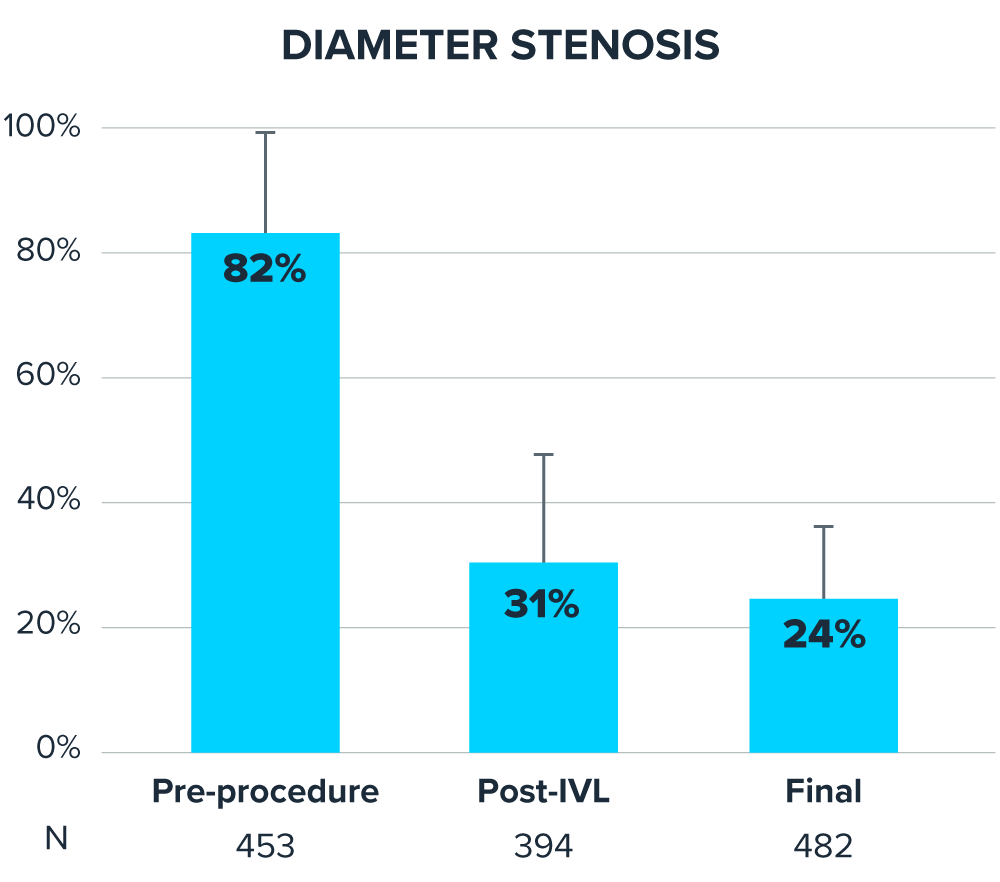
Largest Real-World Experience with Shockwave IVL in Chronic Limb-Threatening Ischemia (CLTI) Patients1
DISRUPT PAD III Observational Study Sub-Analysis of 1,373 patients
Statistics Callout
This section presents key statistical information with numbers and descriptions.
-
450Patients with CLTI
-
543Lesions
-
87%Lesions moderate-severe calcification
-
41%Patients on dialysis
-
35%Lesions were chronic total occlusion (CTO)
-
30%Single-vessel or absent runoff
1: Intravascular Lithotripsy for the Treatment of Patients with Critical Limb Ischemia, Peter A. Soukas, MD. Presented at The Amputation Prevention (AMP) Symposium. Chicago, IL. USA, August 2022.
Featured Clinical Evidence Studies
-
Global prospective, multi-center, single-arm study assessing the safety and effectiveness of Shockwave peripheral IVL in treating long, calcified BTK lesions.Peripheral IVL
-
The largest prospective real-world evidence for the treatment of complex, heavily calcified peripheral arterial disease (PAD).Peripheral IVL
-
The largest-ever randomized clinical study of Shockwave peripheral IVL treatment in severely calcified peripheral lesions, out to 24 months.Peripheral IVL
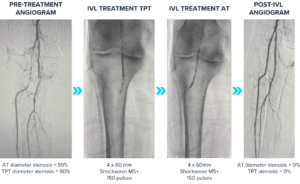
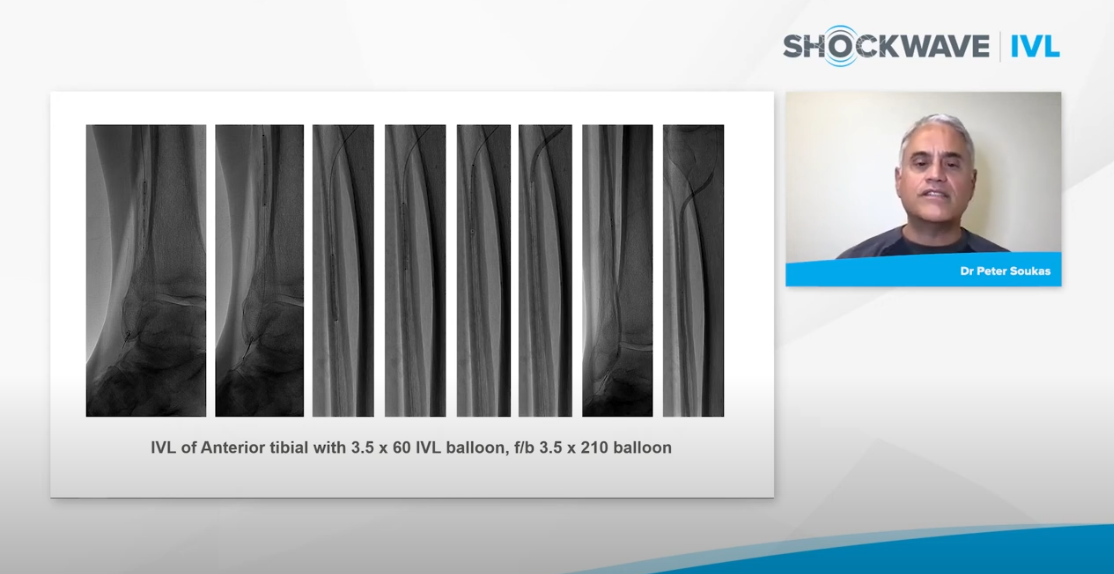
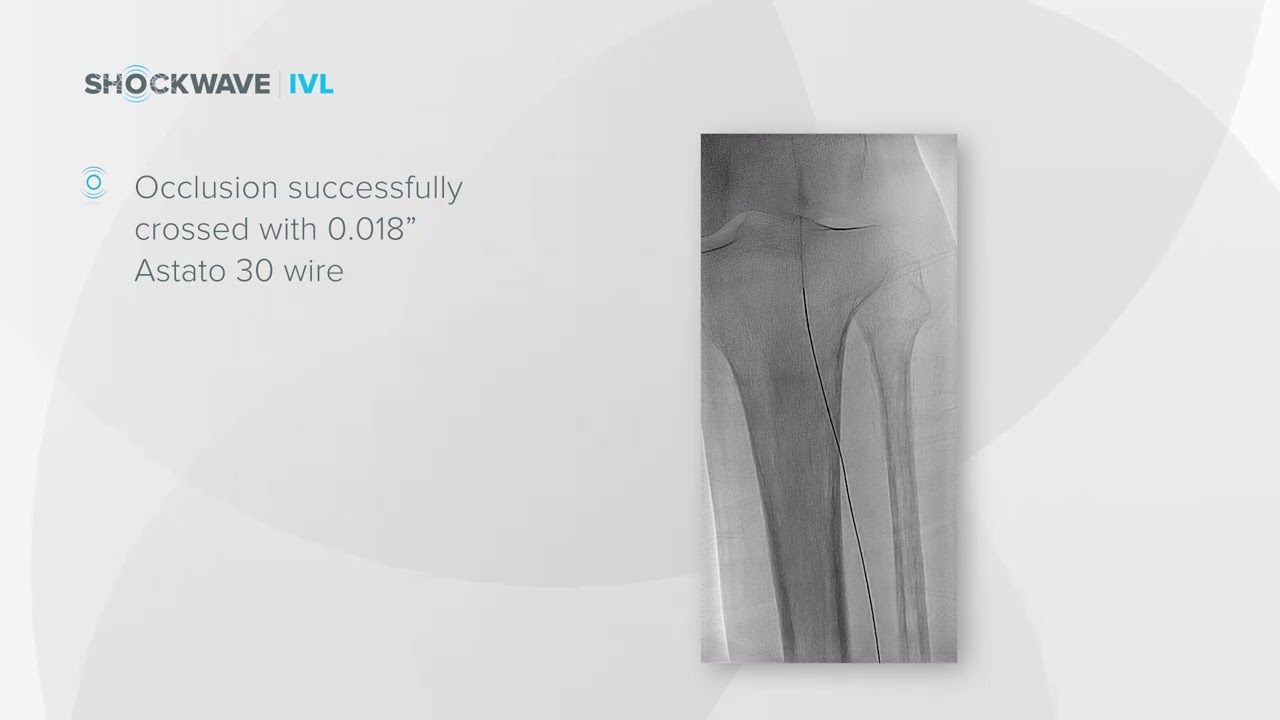
Featured BTK Case: Anterior Tibial Artery (ATA) and Tibioperoneal Trunk (TPT) Disease
An 86-year-old female Rutherford 5 CLTI patient with extensive BTK disease had a medical history that included coronary artery disease (CAD), diabetes mellitus-2, hypertension, hyperlipidemia, end stage renal disease on hemodialysis (HD), former smoker and diastolic congestive heart failure. With a high take-off of the anterior tibial, IVUS showed a reference vessel diameter of 3.5 mm with extensive calcification. A Shockwave M5+ 4.0 mm catheter was used to treat the ATA and TPT for an excellent angiographic result. The follow-up duplex scan showed patency in both the AT and TPT with wound healing at about 4–5 weeks. Case courtesy of Dr. JD Corl.
Go Deeper: Presentations and Case Studies
-

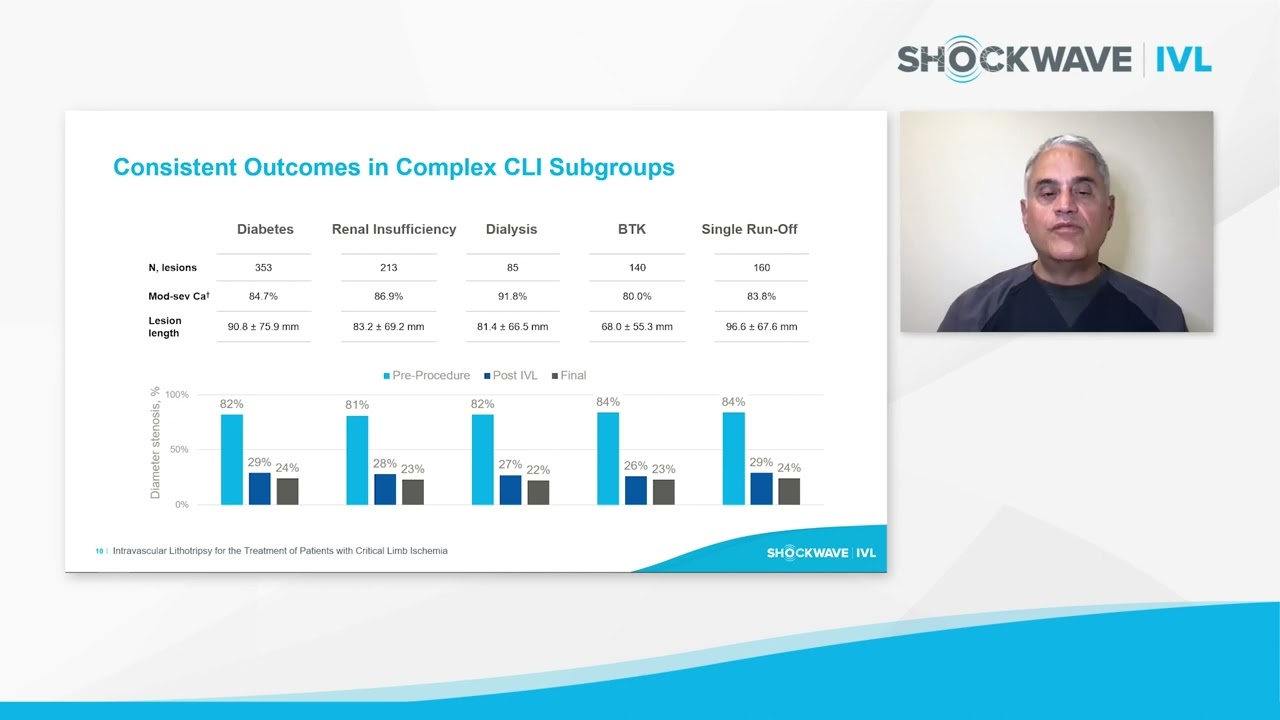
Shockwave IVL for the Treatment of Patients with CLI: Data Presentation
-
Shockwave IVL for the Treatment of Patients with CLI: Interview and Case Examples
-
Dr. Armstrong CLI Case: Nonhealing Wound to Right Great Toe & Non-Compressible ABI
Resources
- Shockwave E8 Tech Sheet
- Shockwave M5+ Tech Sheet
- Safety and Feasibility of Intravascular Lithotripsy for Treatment of Below-the-Knee Arterial Stenoses, Brodmann et al, JEVT, August 2018
- Safe and Effective Treatment of Below-the-Knee Calcium in CLI Patients, by Dr. Sameh Sayfo
- Intravascular Lithotripsy for Critical Limb Ischemia by Dr. Michael Meuse and Dr. Raj Pyne
- Treating Below the Knee Calcium with Dr. Kumar Madassery & Dr. Sabeen Dhand


