Join Dr. JD Corl, Interventional Cardiologist and Medical Director of the PAD/CLI Program at The Linder Center for Research and Education at the Christ Hospital, as he provides an overview of the first-of-its-kind Forward Intravascular Lithotripsy (IVL) Platform, Shockwave Javelin, and reviews three patient cases from the Forward PAD Investigational Device Exemption (IDE) Trial.
First, Dr. Corl posits the current challenge of crossing tight lesions with traditional therapies such as balloon angioplasty and atherectomy, as well as balloon-based IVL – and that’s where Shockwave Javelin comes in. This new, non-balloon-based IVL catheter features a single distal emitter, designed to crack calcium in front of the catheter tip and facilitate the passing of the catheter through the calcified stenosis.
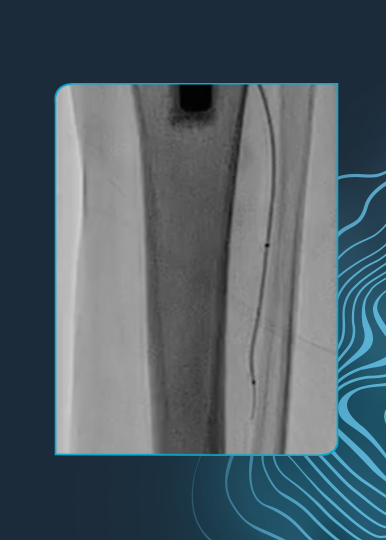
Case Example 1: Right Distal SFA
Dr. Corl’s first patient case is of a 79-year-old male with a history of hypertension, tobacco use, coronary artery disease (CAD) with a history of coronary stenting/bypass and renal insufficiency. The patient had a severe stenosis of the right distal superficial femoral artery (SFA).
After successfully crossing the lesion, post dilation with a percutaneous transluminal angioplasty (PTA) balloon resulted in residual stenosis of 20% with no dissection or embolic complications. The destination therapy used was a 6.0 x 150 drug-coated balloon (DCB) resulting in residual stenosis of 15.49%.
Case Example 2: Left Proximal Posterior Tibial Artery
In the second patient case, Dr. Corl reviews a 51-year-old male with a history of hypertension, type II diabetes, CAD, renal insufficiency and atrial fibrillation, and who had been hospitalized within the prior 60 days for gangrene. The patient had critical limb threatening ischemia (CLTI) of the left foot, with a chronic total occlusion (CTO) of the left posterior tibial artery.
After successfully crossing the lesion, post dilation with a 3.0 x 120 mm PTA balloon resulted in residual stenosis of 3% with no dissection or embolic complications. No destination therapy was used.
Case Example 3: Left Mid Anterior Tibial Artery
The final patient case was of an 85-year-old female with a non-healing ulcer of the left foot and a history of hypertension, hyperlipidemia, tobacco use, type II diabetes, myocardial infarction (MI) and CAD with a history of coronary stenting/bypass and atrial fibrillation with a permanent pacemaker in situ. The patient had a CTO of the left mid anterior tibial artery.
After successfully crossing the lesion with Shockwave Javelin, post dilation with a 2.5 mm x 100 mm PTA balloon resulted in residual stenosis of 18% with no dissection or embolic complications.
Dr. Corl is a paid consultant of Shockwave Medical. Views expressed are those of the authors and not necessarily those of Shockwave Medical.
Shockwave IVL: In the U.S.: Rx only. Prior to use, please reference the Important Safety Information for more information on indications, contraindications, warnings, precautions and adverse events.