See Calcium, Think CALC
Help determine when Shockwave Intravascular Lithotripsy (IVL) might be an appropriate treatment for calcific coronary artery disease with CALC.
Step 1: Determine if compliance adequate
Step 2: Determine device selection
Step 3: Determine when IVL is suitable

Calcified coronary lesions are challenging to treat. Several devices are available, but it’s hard to know which to use and when. Existing calcium algorithms are often overly complex, focus only on calcium morphology, and don’t account for other factors that can strongly influence device-related patient safety.
Additionally, Shockwave Coronary Intravascular Lithotripsy (IVL) has a completely different mechanism of action (MOA) and unique safety profile compared to other devices, but it’s not always clear from existing algorithms when to use IVL and why.
To address this, CALC was developed as a tool to help you determine quickly and easily when Shockwave IVL might be appropriate for treating calcific coronary disease.
-

Concentric, eccentric, or nodular
-
Small or large lumen
-
Length and depth
-
Patient safety



Step 1: Determine if compliance adequate
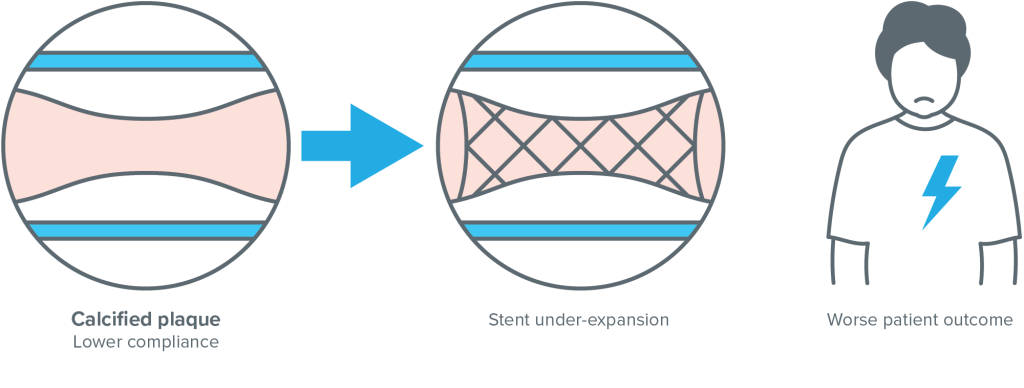
Compliance is a measure of an object’s ability to deform or change shape as pressure is applied. Prior to stent deployment, it’s essential to assess compliance.
- Lesion compliance is a likely predictor of stent expansion which has a major impact on procedural and patient outcomes1,2,3
- Low vessel compliance can be assessed by identifying calcific segments in the lesion which may prevent asymmetrical balloon-expansion at nominal pressure4
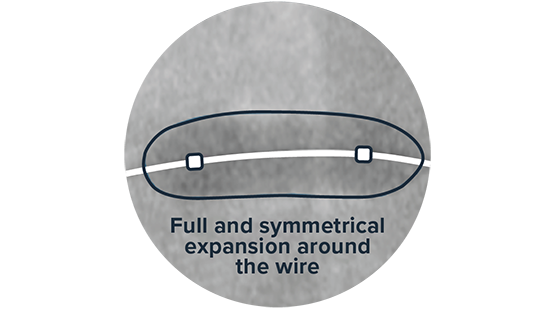
- Adequate balloon expansion is indicated by full and symmetrical expansion around the wire of a 1:1 sized non-compliant (NC) balloon taken to nominal pressure. This should be confirmed in two orthogonal views5
- If compliance is not adequate and a symmetrical expansion cannot be achieved, further calcium modification is recommended prior to stent deployment6
-
Adequate Compliance: Symmetrical Balloon Expansion
Full and symmetrical expansion around the wire -
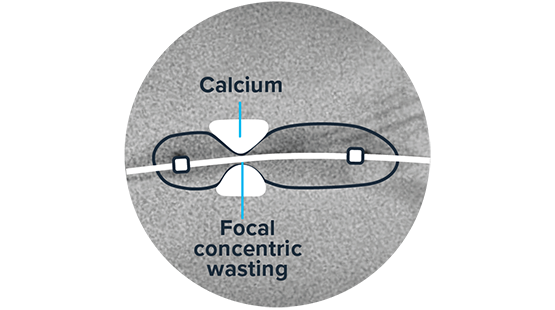
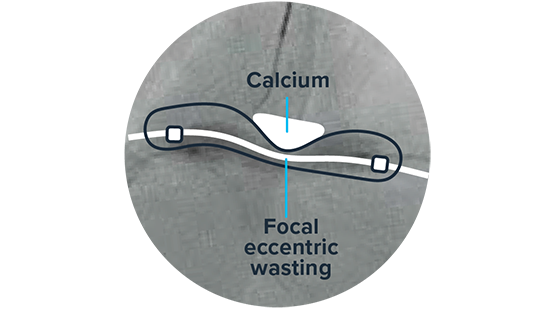
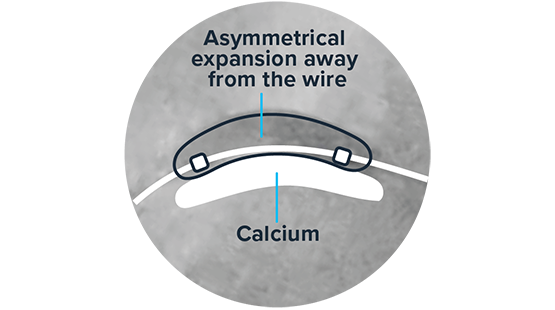
Inadequate Compliance: Asymmetrical Balloon Expansion
No! Concentric calcification -
Inadequate Compliance: Asymmetrical Balloon Expansion
No! Focal eccentric calcification -
Inadequate Compliance: Asymmetrical Balloon Expansion
No! Diffuse eccentric calcification
Step 2: Determine what factors inform device selection
If further calcium modification is required to improve compliance, now’s the time to use CALC to further analyze the calcific lesion(s) and help decide which device to use next.
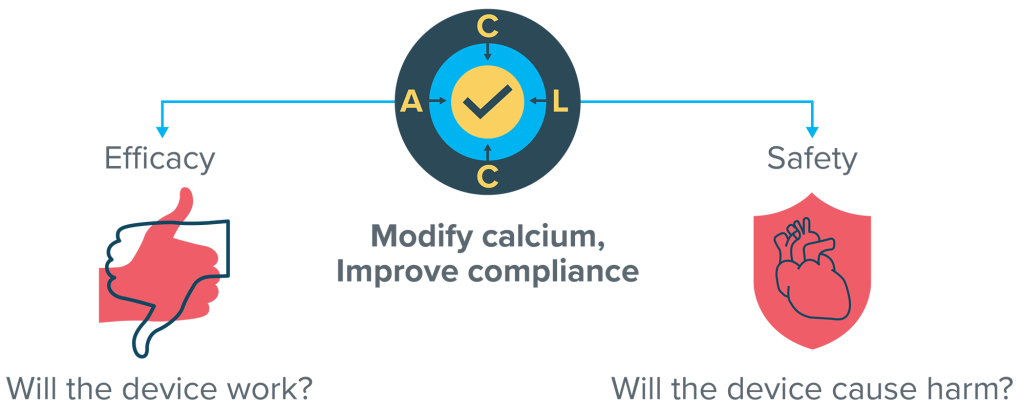
CALC simplifies things into four key factors — Calcium, Area, Length, Complexity — that can strongly influence the efficacy and safety of the different devices and help you quickly determine when Shockwave IVL may be appropriate.
Accordion Section
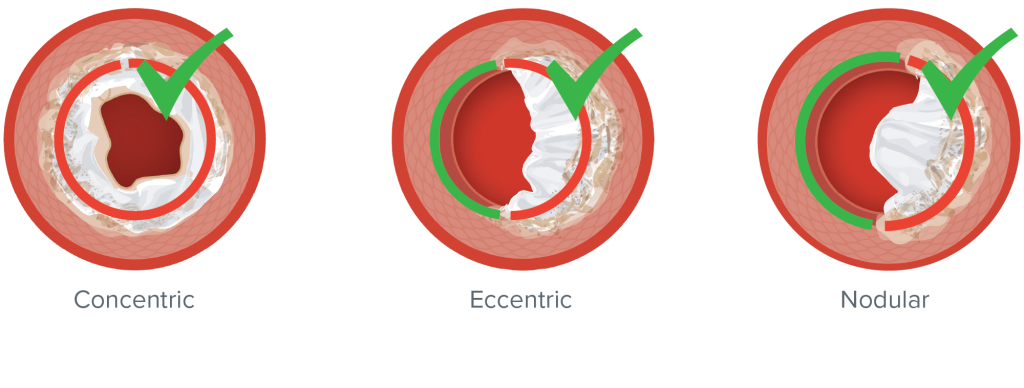
Each type of calcium morphology has a different effect on vessel compliance.
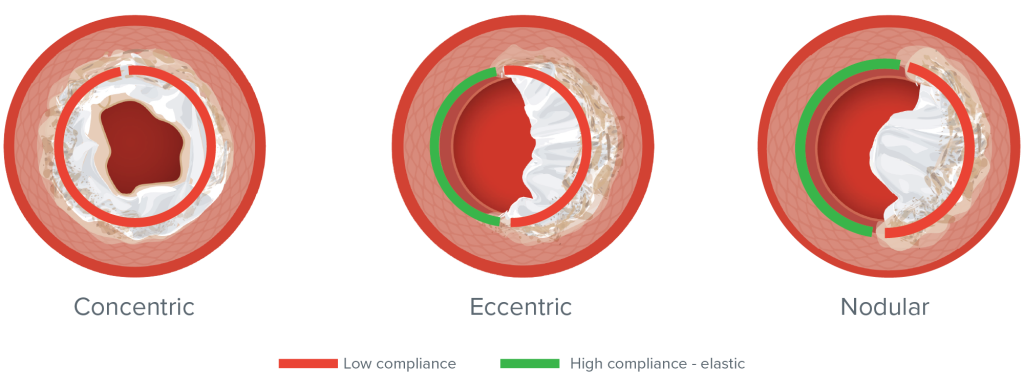
Concentric calcium results in uniform or circumferential low compliance. Eccentric and nodular calcium are characterized by non-uniform compliance with low compliance on one side of calcification and higher compliance on the side without calcium.7
The pattern of compliance can have a major impact on the performance and safety of certain devices:
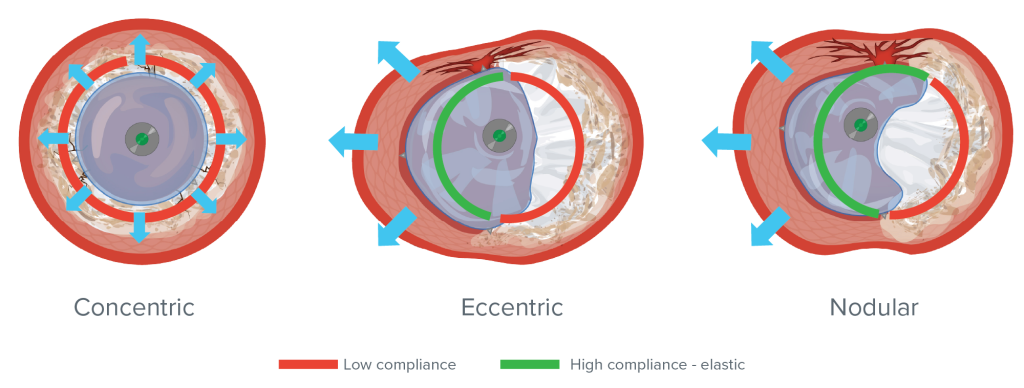
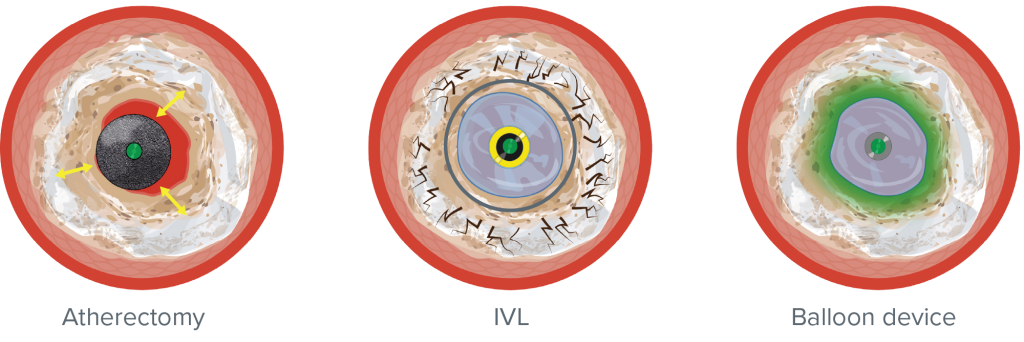
- Balloon-based devices such as NC, open (OPN) or cutting balloons all rely on pressure for their effect, which is not selective for calcium and is not directional8
- In concentric calcium, the force applied is oriented towards the target, because it is circumferential
- In eccentric and nodular calcifications, the force applied will follow the path of least resistance into the high compliance, elastic section of the vessel.8 Luminal gains are often reliant on overexpansion of non-calcific segments — and as pressure is increased the risk of vessel injury also increases9
- Neither Shockwave IVL nor atherectomy devices rely on pressure for their effect6
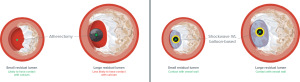
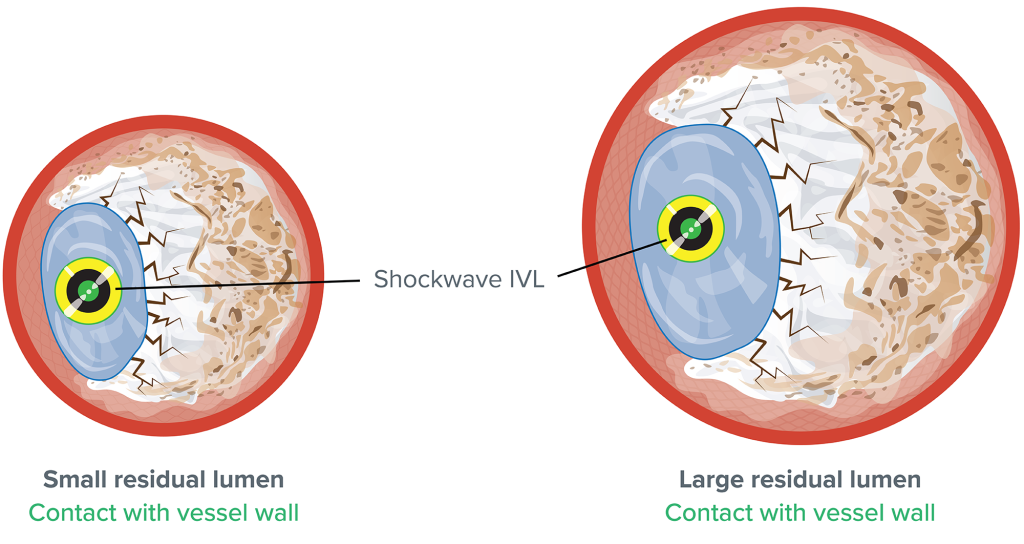
Residual lumen size (among other factors) is important when it comes to device selection because of how it can impact the position of the guidewire relative to the lesion,10 a phenomenon called wire bias.
The larger the actual residual lumen is, the higher the likelihood of the guidewire being positioned away from the calcified section of the vessel wall. Atherectomy devices are contact-dependent when debulking and thus very sensitive to wire bias.6
- In larger residual lumens, atherectomy devices — tracking over the guidewire — are less likely to have contact with the calcified vessel wall. If this is the case, they may have minimal, if any, impact in debulking but still pose a potential risk of damage to healthy vessel segments11,12,13
- Lumen size has little or no impact on the performance of Shockwave IVL or balloon-based devices — if sized correctly11,12,13
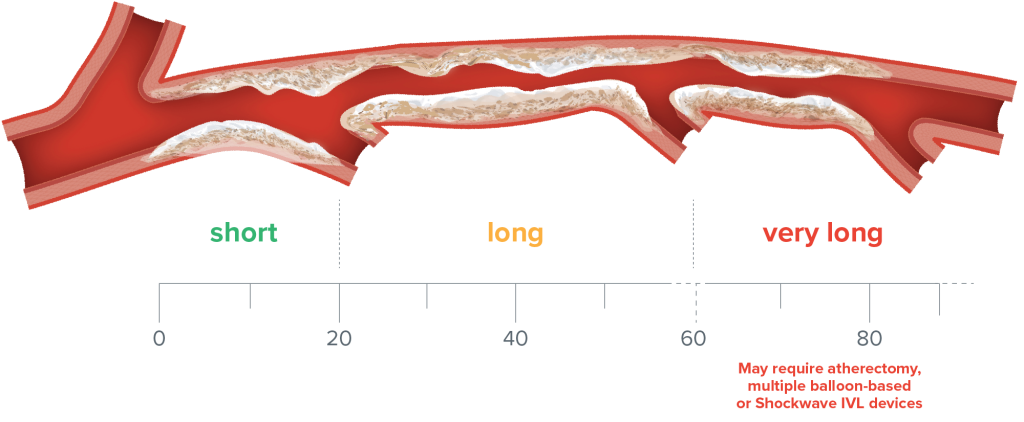
The length and depth of calcific lesions can impact the performance of different devices:
- Calcified lesions vary in length from short (<20 mm) to long (>20 mm)14
- Very long calcified lesions – those longer than 60 mm – may require atherectomy or multiple ballon-based or Shockwave IVL devices to facilitate adequate modification*
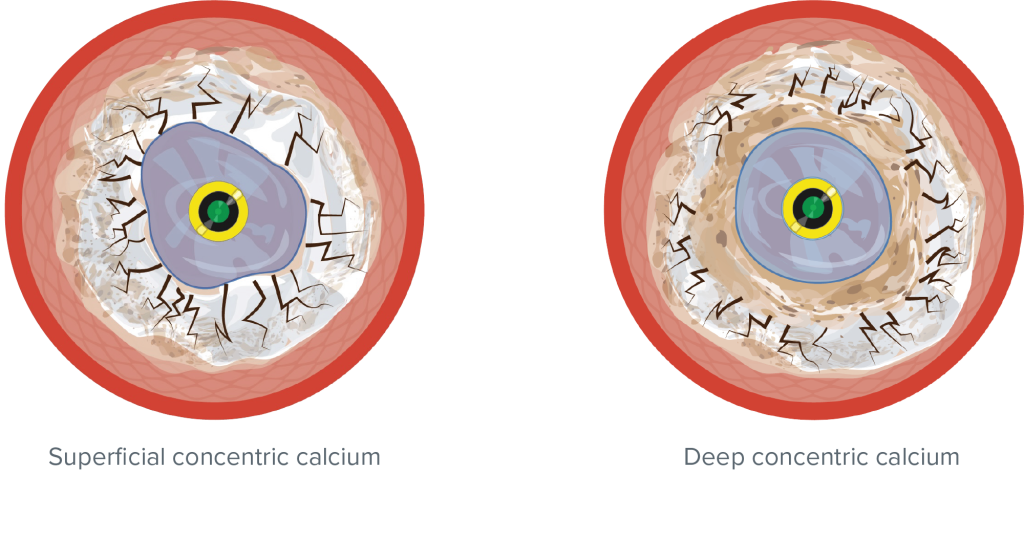
- Coronary calcium depth is important because of how it impacts the performance of different devices6
- Neither atherectomy systems nor balloon-based devices may be able to modify deeper calcium – given their mechanisms of action15
- Shockwaves created by Shockwave IVL pulses are able to travel though the vessel into deep layers of the wall6
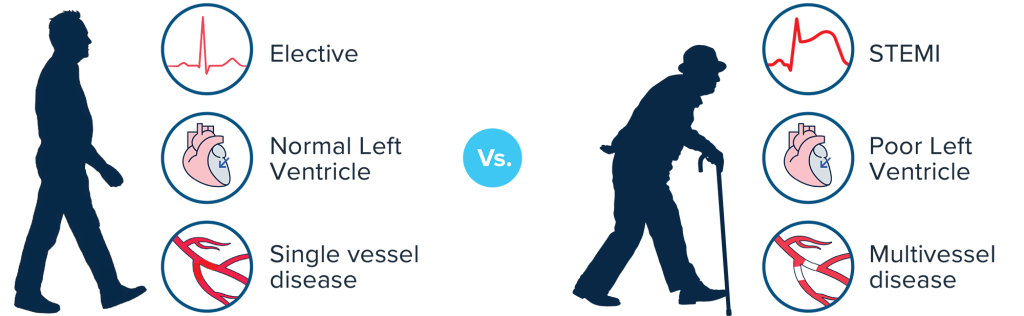
Complications and comorbidities can have serious consequences, so for each calcium modification device under consideration, we must ask ourselves two important questions:
- What is the risk of a complication occurring?
- What is the risk to the patient if it occurs?
The risk of a complication occurring is not the same as its consequence or tolerability for the individual patient. Consider all the other factors that can and do strongly influence the safety of using a specific device for a complex percutaneous coronary intervention (PCI) in a specific lesion for a specific patient, such as:
- Lesion-specific factors:
- Calcium assessment
- Lesion location
- Patient-specific factors:
- Presentation
- Comorbidities
- Left ventricle (LV) function
- Valve disease
![]()
![]()
What if slow flow or a perforation were to occur in either of these patients?
All relevant factors that may influence the safety of electing a revascularization strategy and device for a lesion in a specific patient need to be considered.
Step 3: Determine when IVL is suitable
Shockwave IVL’s unique MOA and proven safety, effectiveness and ability to modify all types of calcium make it a good candidate for calcium modification in many scenarios.16,17,18
Properties of Shockwave IVL:
- Highly selective for calcium
- Effect is not dependent on high pressure inflations
Accordion Section
Shockwave IVL has consistent efficacy data across all calcium morphologies — deep concentric, eccentric and nodular.
Shockwave IVL is not affected by wire bias and is effective in small or large residual vessel lumen.11,12,13
Shockwave IVL can be used for the treatment of short and long lesions as determined by the number of pulses available and the personal pulse management strategy along the calcified areas.*
Very long confluent calcium may require multiple Shockwave IVL devices or an alternative device. However, if the calcium is diffuse and presents itself in different calcium morphologies, Shockwave IVL may be the most effective and safest device to treat the whole lesion,16,17 while using an additional catheter should be considered.
Reminder: Very long lesions more than 60 mm long may require multiple Shockwave IVL devices.
Because Shockwaves are able to travel through the vessel wall, Shockwave IVL can reliably modify calcium irrespective of the depth.16,17,18
Patient safety is paramount and has to be at the forefront of decision-making during any PCI procedure. Shockwave IVL’s unique safety profile plays an important role in high-risk patients.18,19,20
Summary
If balloon-expansion is asymmetrical, the type of calcium, the area, length and depth of calcium, and case complexity, all have a major influence on the performance and safety of Shockwave IVL.
When is Shockwave IVL suitable?
-
Calcium (concentric, eccentric or nodular)
IVL has consistent efficacy data across all calcium morphologies – deep concentric, eccentric and nodular -
Area (small or large lumen)
IVL is not affected by wire bias and is suitable for small and large vessel lumen -
Length (length & depth)
IVL can be used for the treatment of long lesions defined by the number of pulses available. It’s effective in superficial and deep calcium -
Complexity (patient safety)
IVL’s unique safety profile makes it a valuable option for complex lesions and high-risk patients
*See Shockwave C2+ IFU. Do not exceed more than 80 pulses per 12 mm. Available balloon sizes 2.5-4.0 mm.
1: Kobayashi Y, Okura H, Kume T, et al. Impact of target lesion coronary calcification on stent expansion: an optical coherence tomography study. Circ J. 2014;78(9):2209-2214.
2: Prati F, Romagnoli E, Biccirè FG, et al. Clinical outcomes of suboptimal stent deployment as assessed by optical coherence tomography: long-term results of the CLI-OPCI registry. EuroIntervention. 2022;18(2):e150-e157.
3: Bourantas CV, Zhang YJ, Garg S, et al. Prognostic implications of coronary calcification in patients with obstructive coronary artery disease treated by percutaneous coronary intervention: a patient-level pooled analysis of 7 contemporary stent trials. Heart. 2014;100(15):1158-1164.
4: More RS, Brack MJ, Gershlick AH. Angioplasty balloon compliance: can in vivo size be predicted from in vitro pressure profile measurements? Clin Cardiol. 1996;19:393-397.
5: Maffey MW, Bagur R. Balloon techniques for coronary calcium modification. Interv Cardiol. 2024;19:e13.
6: Barbato E, Gallinoro E, Abdel-Wahab M, et al. Management strategies for heavily calcified coronary stenoses: an EAPCI clinical consensus statement in collaboration with the EURO4C-PCR group. Eur Heart J. 2023;44(41):4340-4356.
7: Alfonso F, Macaya C, Goicolea J, et al. Determinants of coronary compliance in patients with coronary artery disease: an intravascular ultrasound study. J Am Coll Cardiol. 1994;23:879-884.
8: Song X, Adachi T, Kawase Y, et al. Efficacy of the Wolverine cutting balloon on a circumferential calcified coronary lesion: bench test using a three-dimensional printer and finite element simulation. Cardiovasc Interv Ther. 2021.
9: Malhotra G, Ong GA, Wilson S, Spratt JC. Eccentric balloon expansion predicts coronary artery perforation: integrating angiography and intravascular imaging. J Am Coll Cardiol. 2024;84(18 Suppl B):B267.
10: Oda T, Kinoshita Y, Miyahara M, et al. Wire bias modification with reverse orbital atherectomy for safer rotational atherectomy in calcified bifurcation. J Cardiol Cases. 2024;29(3):128-131.
11: Blachutzik F, Meier S, Weissner M, et al. Coronary intravascular lithotripsy and rotational atherectomy for severely calcified stenosis: results from the ROTA.shock trial. Catheter Cardiovasc Interv. 2023.
12: Lee T, Ashikaga T, Nozato T, et al. Predictors of coronary artery injury after orbital atherectomy as assessed by optical coherence tomography. Int J Cardiovasc Imaging. 2023;39:1367-1374.
13: Kawaguchi Y, Tamura T, Masuda S, et al. Impact of the degree of wire bias in the vessel’s healthy portion on coronary perivascular trauma in rotational atherectomy. Cardiovasc Revasc Med. 2022;40:123-131.
14: Scarsini R, Fezzi S, Leone AM, et al. Functional patterns of coronary disease: diffuse, focal, and serial lesions. JACC Cardiovasc Interv. 2022;15:2174-2191.
15: Oomens T, Vos NS, van der Schaaf RJ, et al. Expansion of stents after intravascular lithotripsy versus conventional predilatation in calcified coronary arteries. Int J Cardiol. 2023;386:24-29.
16: Kereiakes DJ, Virmani R, Hokama JY, et al. Principles of intravascular lithotripsy for calcific plaque modification. JACC Cardiovasc Interv. 2021;14(12):1275-1292.
17: Ali ZA, Kereiakes DJ, Hill JM, et al. Impact of calcium eccentricity on the safety and effectiveness of coronary intravascular lithotripsy: pooled analysis from the Disrupt CAD studies. Circ Cardiovasc Interv. 2023;16:e012898.
18: Ali ZA, Shin D, Singh M, et al. Outcomes of coronary intravascular lithotripsy for the treatment of calcified nodules: a pooled analysis of the Disrupt CAD studies. EuroIntervention. 2024;20(23):e1454-e1464. doi:10.4244/EIJ-D-24-00282.
19: Honton B, Cayla G, Lhermusier T, et al. National France LILI registry on intravascular lithotripsy: 30-day follow-up. Arch Cardiovasc Dis. 2024;117(Suppl):S15-S16.
20: Frampton J, Kearney KE, Abbott JD, et al. Coronary intravascular lithotripsy for treatment of severely calcified lesions: long-term sex-specific outcomes. J Soc Cardiovasc Angiogr Interv. 2023;2(6):101069.