A Superior Strategy
For Calcified PAD
IVL provides superior vessel prep and excellent long-term results in calcified vessels while preserving future treatment options
IVL provides superior vessel prep and excellent long-term results in calcified vessels while preserving future treatment options


*Data refers to IVL arm of randomized study
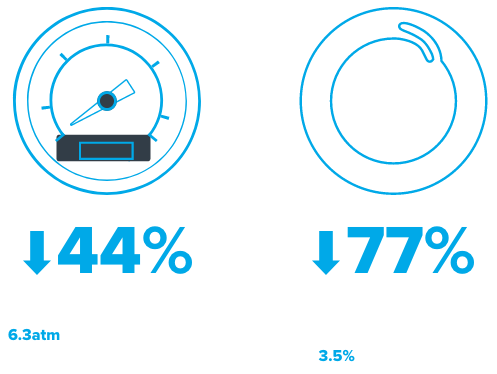
IVL’s unique mechanism of action delivers significantly more luminal gain with lower dilatation pressure and less need for post-dilatation
Superior Procedural Success

Procedural Success = Residual stenosis ≤30% without flow‑limiting dissections prior to DCB +/- stenting
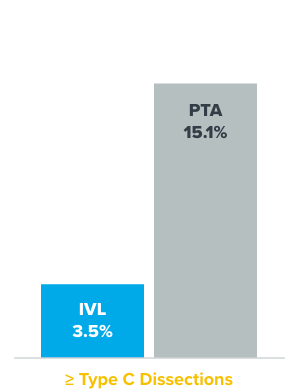
Atraumatic Treatment
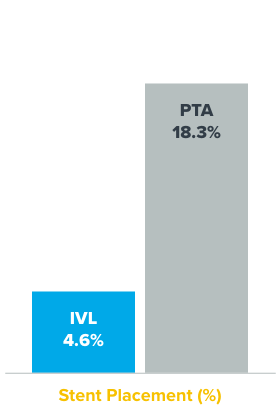
IVL maintains control of the procedure by minimizing complications such as dissections, embolization, and perforations. IVL significantly reduces the need for bailout stents, preserving future treatment options.
Reduced Dissections
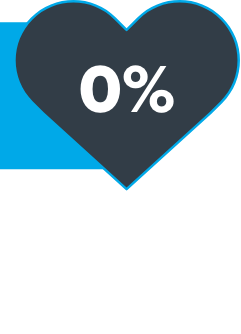
Low Complications
Reduced Bailout Stenting
Embolic protection: Utilized in 1.3% of cases in IVL treatment arm.
Provisional stent: Utilized if residual stenosis ≥50% by visual estimate or unresolved ≥ type D dissection, and trans-lesional gradient > 10 mmHg
IVL has demonstrated excellent patency out to two years in a severely calcified patient population
Primary Patency*
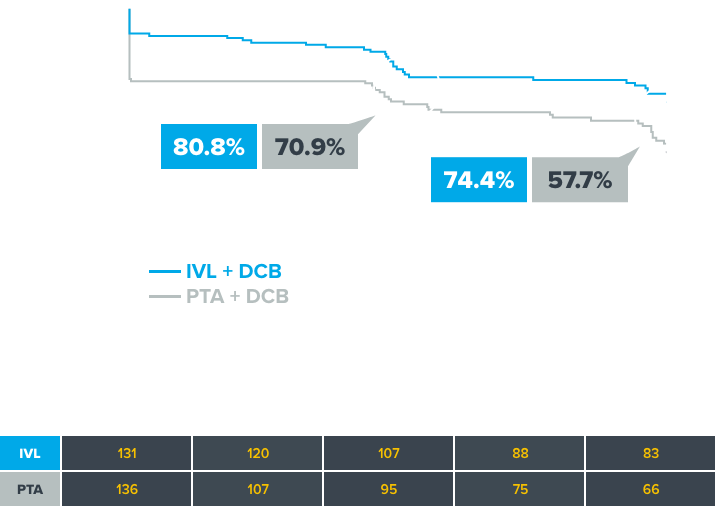
*Primary Patency defined as freedom from provisional stenting at index procedure, freedom from clinically-driven target lesion revascularization, and freedom from restenosis determined by duplex ultrasound


See how the new faster, further, larger Shockwave M5+ can help treat your patients with calcified PAD
LEARN More
Looking for careers? Click here.